At MedPAC’s October public meeting, the Commission had a session that focused on how Medicare can get the payment rates right in its fee schedule for physicians, nurses, and allied health professionals.
Context: for years, the Commission has been concerned that certain services, such as primary care, are undervalued in the fee schedule relative to other services. Case in point, a MedPAC analysis shows that if physicians were paid entirely on Medicare rates, orthopedists would be paid $392,000 – more than double family medicine doctors. The long-run concern is that due to lower reimbursement rates, fewer will opt to enter primary care. The Commission believes that primary care is the backbone of a well-functioning, coordinated delivery system, so underpaying primary care could have the effect of undermining coordinated care. The Commission has made a host of recommendations over the years for supporting primary care through Medicare payment policy, including several as part of a package to reform Medicare’s Sustainable Growth Rate.
A little more background: Payments to physicians and other health professionals in Medicare are determined by a fee schedule, containing about 7,000 services. Each service is assigned a “relative value,” which determines how much Medicare pays for the service. (MedPAC’s payment basics summarizes how this works in more detail.) The relative values are constructed based on several factors, and one of the most important is the time it takes to perform the service. If the estimates in the fee schedule of how long it takes to provide a service are incorrect, then the service will be priced incorrectly.
In 2011, as part of its SGR reform package, the Commission recommended that CMS undertake a data collection effort to help identify services in the fee schedule that are mispriced, so that corrections can be made. CMS now has a statutory mandate and the resources to examine and address inaccuracies in the fee schedule. They currently have a few contracts underway, both which have taken a “bottom up” approach, meaning they attempting to validate the time estimates for services one-by-one. This process may require direct observation or time-and-motion studies, or detailed data from electronic health records. This is likely to be burdensome for providers and CMS, potentially biased, and very costly. Because of the burden and cost, it is unlikely that the approach could be repeated regularly to maintain accuracy over the long term.
The Commission is exploring a different approach. Instead of looking at each individual service “bottom-up,” the “top-down” approach looks at the amount of time that a physician worked over the course of a day/week/month and compares it to the fee schedule time estimates inherent in all the services that the physician billed over that same time period. If a physician worked 10 hours, but the fee-schedule time assumed that the services furnished required 15 hours, this might suggest that the time estimates in the fee schedule are overstated. Statistical analysis of the data would then provide direction for further investigation by CMS.
A contractor for MedPAC explored the feasibility of this approach by collecting data from a small set of physician practices on the services that its practitioners billed (by CPT code), as well as practitioner’s actual hours worked. They looked at data for four practices—cardiology, family medicine, orthopedics and urology. The chart below shows the results.
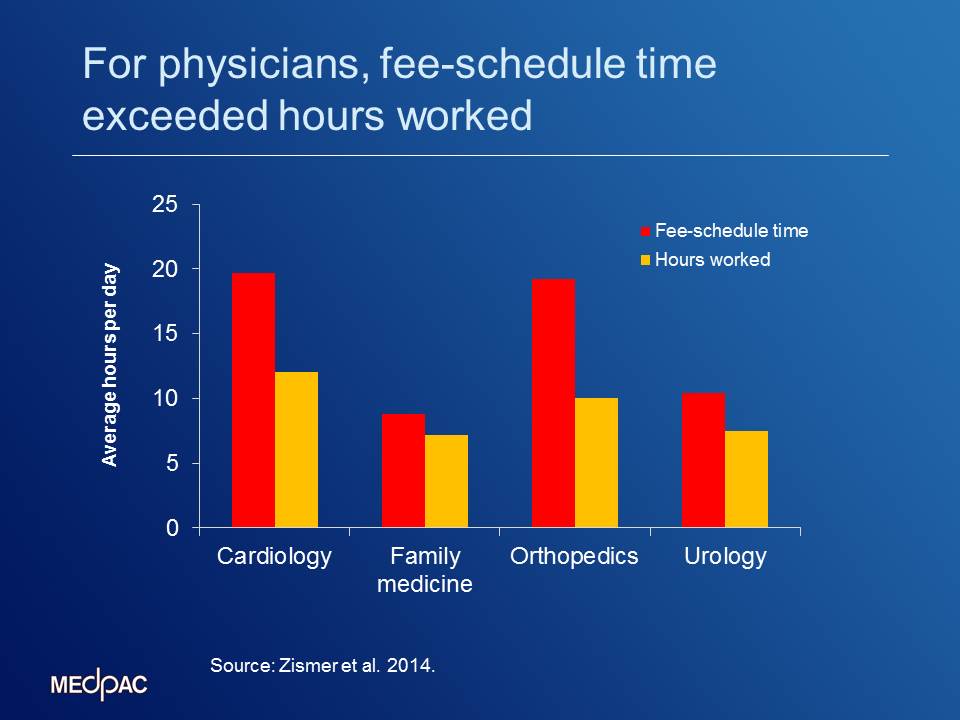
Computing averages for each of the practices, the contractor found that, for physicians in all of the practices, fee-schedule assumed time exceeded actual hours worked (see chart). For the physicians in the family medicine practice, the difference was smallest, with fee-schedule time averaging 8.8 hours per day but hours worked per day averaging 7.1 hours, a difference of 24 percent. For the physicians in the orthopedics practice, the difference was the largest among the four practices, with fee-schedule time averaging 19.2 hours per day but hours worked averaging 10.0 hours per day, a difference of 92 percent. This would suggest that services provided by the orthopedic practice may be based on inflated time estimates, and further investigation of the relative values for these services may be needed.
Caveat: These data represent a small number of practices and physicians and are not definitive. The task of collecting enough data to reliably conduct this analysis has its challenges. However, these provisional findings are directionally consistent with the Commission’s concerns – that primary care services are undervalued in the fee schedule and procedural and testing services are overstated. The vast majority of fee-schedule time for the physicians in the family medicine practice is time furnishing office visits. By contrast, the physicians in the other three practices—where the differences between fee-schedule time and hours worked are larger and they provide more imaging, procedural, and testing services.
The Commission’s discussion is intended to inform the Congress and CMS about the feasibility and potential advantages of the “top-down” to correcting inaccuracies in the fee schedule for physician services. This approach could be a desirable method for ensuring the accuracy of the fee schedule going forward and to do so in a way that is more efficient than trying to validate the RVUs for each individual service.